Approximately 9% of men and 24% of women will experience migraine headache. The 2010 Global Burden of Disease Survey lists migraine as the 7th highest cause of disability. Those affected with the condition can experience a significantly decreased quality of life—something to which readers who have experienced these crippling headaches can attest. After having spent my fair share of time lying in bed, lights off, begging loved ones to keep the noise down, I can honestly say that if I never have another migraine again, it will be too soon!
Migraine is described as a recurrent disorder, typically lasting between 4-72 hours. Characteristics include unilateral location, pulsating quality, aggravation by physical activity, nausea and vomiting, and light and sound sensitivity. A subset of patients may experience sensory symptoms such as flashing lights, changes in smell, or difficulty speaking.
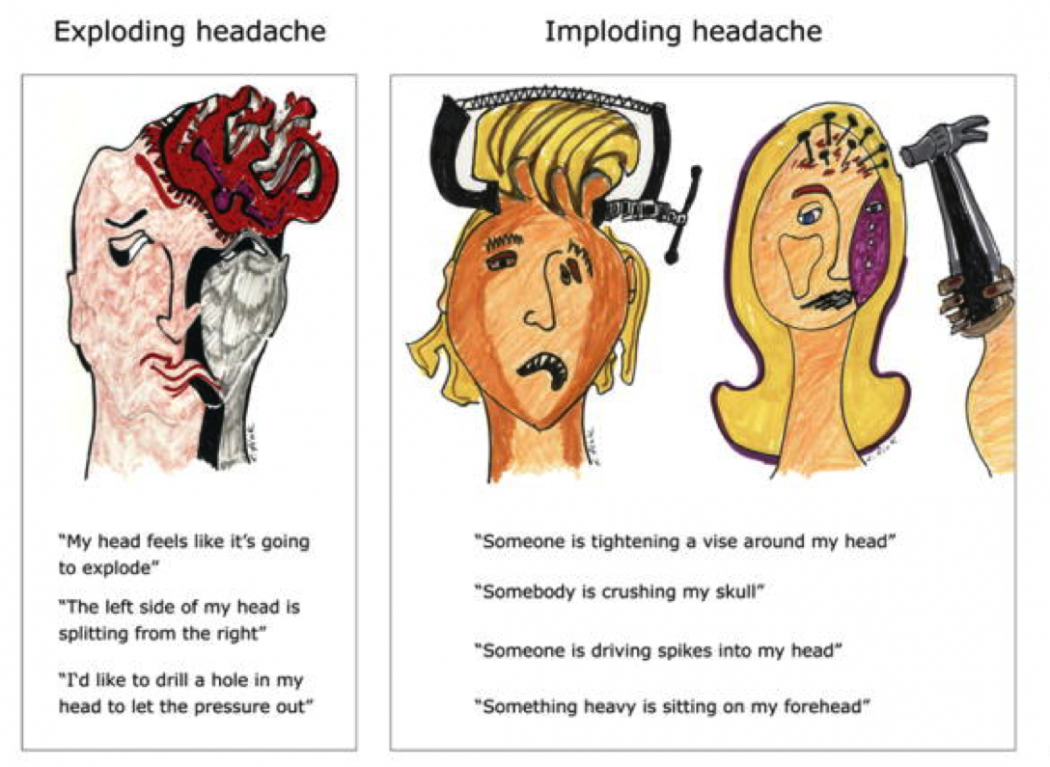
 Treatments for migraine vary greatly, from the “triptans,” a group of medication specifically targeted for migraine, to beta-blockers and antidepressants. One treatment option uses a series of Botox injections at 31 different points on the head. While this may be incredibly effective in some patients, other patients experience virtually no change in symptoms. Jakubowski et al. set out to determine why certain populations responded positively to Botox treatment, while others showed no improvement [1]. After comparing the groups, it appears that the quality of headache pain has a significant correlation to the response to Botox treatment. The group that responded positively to Botox was found to have “imploding” headaches that were described with phrases such as “somebody is crushing my skull” or “somebody is driving spikes into my head.” Alternatively, the group that did not respond to Botox was found to have “exploding” headaches, using phrases such as “my head feels like it is going to explode” or “I’d like to drill a hole in my head to let out the pressure.”
Treatments for migraine vary greatly, from the “triptans,” a group of medication specifically targeted for migraine, to beta-blockers and antidepressants. One treatment option uses a series of Botox injections at 31 different points on the head. While this may be incredibly effective in some patients, other patients experience virtually no change in symptoms. Jakubowski et al. set out to determine why certain populations responded positively to Botox treatment, while others showed no improvement [1]. After comparing the groups, it appears that the quality of headache pain has a significant correlation to the response to Botox treatment. The group that responded positively to Botox was found to have “imploding” headaches that were described with phrases such as “somebody is crushing my skull” or “somebody is driving spikes into my head.” Alternatively, the group that did not respond to Botox was found to have “exploding” headaches, using phrases such as “my head feels like it is going to explode” or “I’d like to drill a hole in my head to let out the pressure.”
This novel concept of describing headaches based on their quality, now termed “headache directionality,” is believed to have clinical implications regarding migraine treatment. It may help to guide physicians when deciding the best treatment options for their patients, directing patients with “exploding” headaches towards treatment options that may be more effective than Botox. However, for this knowledge to be useful to clinicians, a standardized method of determining headache directionality must be determined.
Many patients have never been asked about the quality of their migraine pain in terms of “exploding” or “imploding.” As such, they often find it difficult to answer these kinds of questions accurately. My scholarly project is looking at different methods of determining headache directionality in the hopes of forming a standardized clinical protocol. The study will have patients answer questions about their migraine pain using several different formats. One method will use a pictorial representation in which the patient can choose the picture that best matches his or her own experience with headache pain. Another method will involve written descriptions that the patient can choose to identify his or her pain. For example:
“A sensation of pain or pressure that builds from within and feels as if your head is expanding outward, pushing out from the inside.”
or
“A sensation of pain or pressure that builds from the outside and feels as if your head is pressing inward, pushing in from the outside.”
Finally, a headache neurologist will interview the patients and make an assessment of their headache directionality, based on patient answers to standardized questions. These three methods of questioning will all be compared to a 30-day headache diary, in which patients will record all of their headaches along with their “type”—pushing in or pushing out. This headache diary will be used as the gold standard, as it seems reasonable to assume that patients can most accurately describe their headaches in the moment. Once the diary is completed, it will be compared to the three methods of questioning (pictorial assessment, written description, and physician interview). It is the goal of the project to determine if one technique will prove to be most sensitive and specific for predicting migraine directionality. This method can then be used in the clinical setting when evaluating a patient with migraine, and the physician can therefore forego the use of a headache diary when characterizing migraine to create the optimal therapy regimen.
- Jakubowski M, McAllister PJ, Bajwa ZH, Ward TN, Smith P, Burstein R. Exploding vs. imploding headache in migraine prophylaxis with Botulinum Toxin A. Pain. 2006;125(3):286-295. doi:10.1016/j.pain.2006.09.012
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013 Jul;33(9):629-808 full-text

Carmen Hoffman is a medical student in the Class of 2018. She is a native of Arizona and attended Arizona State University, where she received a Bachelor of Arts in philosophy. When she has finished school (in the far, far-off future), she hopes to pursue a career in medical ethics. To contact Carmen, please e-mail her at carmenhoffman[at]email.arizona.edu.