Welcome to our very first edition of This Month in Science (TMIS). Each month, we will feature recently published research with interviews of our Phoenix faculty for their opinions and explanations. This month, we interviewed Dr. Mark Haussler, who needs no introduction. We are lucky to have Dr. Haussler at UA COM-P and so grateful that he agreed to participate for our first edition! Enjoy!
THIS MONTH IN SCIENCE…
We learned that evolocumab, a monoclonal antibody inhibiting proprotein convertase subtilisin-kexin type 9 (PCSK9), reduces low-density lipoprotein (LDL) cholesterol levels.
As we (newly minted) MS2s know from the illustrious Dr. Haussler—a PCSK9 inhibitor, or neutralizer—is the hot new drug for cholesterol control [1]. Studies so far, however, have been mostly short-term and thus the long-term side effects and true effectiveness of the drug have not been well elucidated. In April, the New England Journal of Medicine published the results of a year-long phase 3, randomized, controlled trial examining the use of evolocumab in addition to standard therapy compared to standard therapy alone [2]. Their results confirmed previous reports on the benefit of evolocumab, as the addition of evolocumab to standard therapy significantly altered lipid profile and was associated with a reduction in cardiovascular events.
We spoke with our very own expert on cholesterol—Mark Haussler, PhD—on what this study means for the future of cholesterol therapies.
YAEL KUSNE, MS2: Dr. Haussler, thank you for agreeing to participate in “This Month in Science!” It’s an exciting new monthly look at clinical research from the perspective of our community scientists and clinicians. We are lucky to have you here! Unfortunately, the MS1s won’t get the pleasure of your hilarious and extremely informative lectures next year. Is that correct that you won’t be lecturing this year?
DR. HAUSSLER: Not quite. It is true that I will be retiring next spring and won’t have the opportunity to lecture to the Class of 2019 in Cardiovascular and Renal although I am sure that they will be exposed by other faculty to the clinical wonders of PCSK9 inhibitors. But it is great that you are covering the latest pharmacologic breakthrough in preventing atherosclerosis and myocardial infarction right here in the new, hot-off-the-keyboard, campus newspaper. Thank you for your interest and greetings to your Class of 2018; I’ll see you in REBLS this Fall. Welcome to the Class of 2019! You will have the dubious pleasure of being exposed to my corny humor and Halloween skeleton costume this Fall in Neuromuscular and Skeletal (NMS) Systems. But let’s get back to evolocumab, the new miracle drug that dramatically lowers LDL (bad) cholesterol.
YAEL: Yes, we wanted to get your take on this study published in the NEJM in April on evolocumab. You told us that PCSK9 blockers were the next big thing in “bad” cholesterol-lowering therapy. You even went so far as to say that “anti-PCSK9 drugs will be as big as statins.” Why do you think that blocking PCSK9 is so successful in altering lipid profiles when used in conjunction with standard statin therapy?
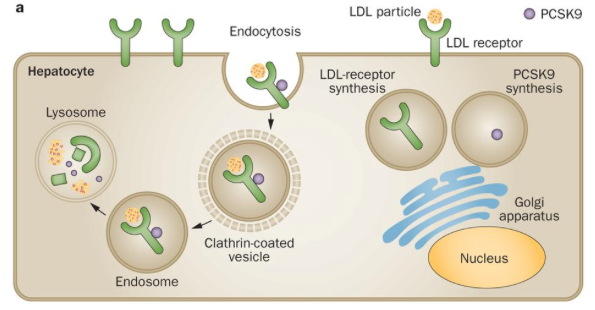
a. PCSK9 is synthesized in the liver as an inactive enzyme precursor that contains a triad of residues required for catalytic activity. PCSK9 circulates in the plasma as a phosphoprotein and, after having been secreted, can immediately bind to, and be endocytosed with, surrounding LDL receptors. The complex of the PCSK9 molecule and the LDL receptor is internalized and undergoes degradation in endosomal and lysosomal compartments, with few receptors recycled to the cell surface. This leads to a decreased number of LDL receptors on the surface of cells.
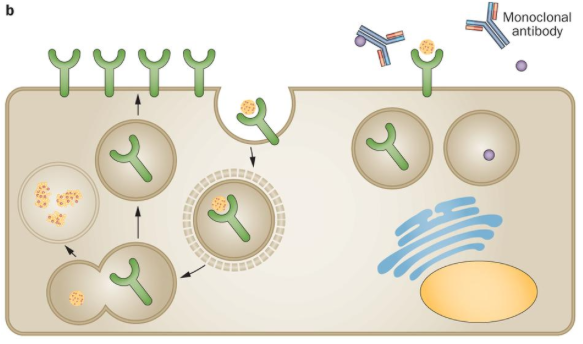
b. Human monoclonal antibodies can bind to PCSK9 adjacent to the region that is required for interaction with LDL receptors. PCSK9 is, therefore, prevented from binding to LDL receptors. After endocytosis, the LDL receptor is recycled back to the surface of the cell, with few receptors degraded in the lysosome. Abbreviation: PCSK9, proprotein convertase subtilisin/kexin type 9.
DR. HAUSSLER: PCSK9 is a molecular relic of the tough times when cholesterol was scarce and during the Spartan periods when saturated fat was a delicacy instead of in cheap supply at the corner fast-food joint. Primitive humans and other animals needed cholesterol in their circulation to deliver it to all cells in the body for membrane integrity and to those endocrine organs that synthesize steroid hormones, which allow adaptation to the environment as well as propagation of the species. To ensure that precious cholesterol carried by LDL wasn’t cleared by the liver via LDL receptors, the cholesterol guardian PCSK9 evolved as a LDL receptor trap that captured surface LDL receptors and removed them to preserve circulating LDL cholesterol. All was well and good until excess refined sugar and saturated (or worse, trans) fat flooded the kitchens of first-world countries. Resulting excess circulating LDL cholesterol now becomes pathogenic and deposits in artery walls of patients who are overweight, obese, and/or have type II diabetes. Statins are an effective way to lower LDL cholesterol and became blockbuster drugs that function by inhibiting cholesterol synthesis (at the HMG CoA-reductase step) from fatty acid fragments and from glucose. When statins inhibit cholesterol synthesis in liver, this induces the formation of more LDL receptors to be placed on the cell surface. Normally, this would be a good thing because cholesterol would be cleared more efficiently. However, the newly minted LDL receptors in patients on statins don’t make it to the cell surface and don’t remain there because they are intercepted or captured by PCSK9. Therefore PCSK9 prevents some of the good work done by statins. Big Pharma reasoned that if they could inhibit PCSK9, not only would statins work better, but by maintaining LDL receptors on the surface of liver (and other) cells, tissues would behave like giant LDL vacuum cleaners to suck bad LDL cholesterol out of the circulation and preclude its deposition in artery walls. Indeed, evolocumab monoclonal antibodies immunoneutralize PCSK9 to take it out of the equation. This means that statins and evolocumab represent the ultimate one-two punch for lowering LDL cholesterol and the incidence of fatal heart attacks in those patients recalcitrant to statins alone. The reason PCSK9 inhibitors are synergistic with statins is that they work by enhancing cholesterol clearance, whereas statins act in a complementary fashion to inhibit cholesterol biosynthesis. The proof of concept appears in the NEJM article you are featuring and, in my opinion, this one-two punch will knock out (or at least knock down) coronary artery disease in those patients who are genetically or epigenetically vulnerable to high LDL cholesterol levels.
YAEL: Do you think this means that patients will eat that chicken-fried steak with a side of waffles for breakfast because they think their doctors will fix their cholesterol with drugs?
DR. HAUSSLER: I hope not! The prevention of heart attack, the number 1 killer of both men and women, requires diligence in diet and exercise, plus lowering LDL cholesterol if the patient is genetically and/or epigenetically predisposed to coronary artery disease. Pigging out (pun intended) on meat from four-legged animals and soaking up sugar are the worst possible things for your patients’ health. Combining these with smoking, obesity, and a sedentary lifestyle is the recipe for disaster. What was rare in antiquity has become a modern pandemic of first-world disease. The physician’s calling is to maintain total health, not just reduce LDL cholesterol to vanishingly small numbers. Thus, to lower the risk of heart attack and ischemic stroke, plus many other diseases such as diabetes mellitus type II, a prudent diet of cold-water fish, vegetables and fruit will do the trick. And why not add dark chocolate in moderation and one glass of red wine to your patient’s lifestyle?
YAEL: You are certainly a role model for us in terms of fitness and health. What do you do to stay healthy and keep your cholesterol in check (besides taking vitamin D)? ☺
DR. HAUSSLER: Basically, my wife, Carol, drags me to the gym to work out with two trainers at least twice a week and prepares only fish, vegetables, and fruit for meals (our pantry is like a health-food store). We walk with our dog four miles a day and make sure we accumulate at least 10,000 steps (Fitbit). Total no-no items are trans fats, French fries, donuts, etc., etc. Neither of us take a statin or PCSK9 inhibitor, and we eat eggs as another source of protein. Increased cholesterol is caused by saturated fat (pathologically alters cholesterol distribution and levels), and sugar, which in excess of caloric requirements, is converted straight to saturated fatty acids and cholesterol. By replacing saturated (and trans) fat with polyunsaturated fatty acids (PUFAs) of marine animals, we maintain a low LDL cholesterol. PUFAs, plus alcohol in moderation and aerobic exercise also raise HDL (good) cholesterol; mine is 59 mg/dL. Of course, the real secret to health and longevity is vitamin D. We supplement with 2000 IU daily. D is not just for the bones, but it also improves mood/mental health, helps fight infections, and lowers the risk of cancer, cardiovascular disease, and autoimmune disorders. With respect to longevity and healthspan, the silent killer is soft drinks/soda pop. The culprit in soda, diet or not, is phosphate. Phosphate zaps the kidneys and leads to calcification of the coronary and cerebral arteries. In short, can the soda!
YAEL: What advice would you give us, as future physicians, in counseling our patients on diet and exercise?
DR. HAUSSLER: Exercise is crucial for health and well-being. Not only is it a mood elevator, but exercise allows your patients’ muscles to burn off fat derived from excess calories that normally would deposit in their fat depots (bellies are the worst). I favor a minimum of 30 minutes of vigorous exercise every day, but this can be accomplished in a number of fitness modalities, depending on the preferences of the patient. It is important that your patients maintain strength, flexibility and endurance as they age. Diet is equally important for health, and your patients are not only what they eat, but because of epigenetics, they are what their mother and father, as well as their grandparents, ate. Because it is too late to put those in one’s family tree on a proper diet, at least until your patient’s epigenome can be edited. The best advice is to eat healthy. I recommend Dr. Andrew Weil’s heart-healthy anti-inflammatory diet. Basically, urge your patients to eliminate processed and fast food, instead consuming whole foods as if they lived on a farm. Advise your patients to consume cold-water fish and poultry, nuts and PUFA/MUFA oils, eggs and whole grains, as well as liberal amounts of fruits and vegetables.
YAEL: Dr. Haussler, it has been a pleasure. Your CV speaks for itself. You are an accomplished, brilliant scientist and professor with a great sense of humor. We love your passion for teaching, and you make no bones about your investment in our success. You’ve taught medical students for 44 (yes, that reads FORTY FOUR) years!! We wish all of our professors would come to class wearing a skeleton outfit. Do you mind if we post a picture of you on Halloween from last year?
DR. HAUSSLER: No problem, it was a fun way to dramatize the skeleton during the NMS block. I look forward to interacting with 2019 in NMS and 2018 in REBLS!!
YAEL: Thank you, Dr. Haussler. CO 2018 can’t wait until REBLS!
 Mark Haussler, PhD, is Regents Professor and Founding Head of the Department of Basic Medical Sciences and the SRP Valley of the Sun Endowed Professor at UA COM-P. He was awarded the Lifetime Teaching Award, among many other accolades for his research and teaching. He is a professor in the Departments of Physiology and Chemistry & Biochemistry and a member of the UA Sarver Heart Center. Dr. Haussler has taught medical students for 44 years.
Mark Haussler, PhD, is Regents Professor and Founding Head of the Department of Basic Medical Sciences and the SRP Valley of the Sun Endowed Professor at UA COM-P. He was awarded the Lifetime Teaching Award, among many other accolades for his research and teaching. He is a professor in the Departments of Physiology and Chemistry & Biochemistry and a member of the UA Sarver Heart Center. Dr. Haussler has taught medical students for 44 years.
You can read about his successful research laboratory here:
http://bms.med.arizona.edu/faculty/mark-r-haussler-phd
You can read about his love of family, life, bones, and Hawaiian shirts here: http://phoenixmed.arizona.edu/news/faculty-spotlight-mark-haussler-phd
References:
- Dadu & Ballantyne (2014). Lipid lowering with PCSK9 inhibitors. Nature Reviews Cardiology 11: 563-575.
- Sabatine, MS, et al (2015). Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. NEJM, 372: 1500-1509.
Yael Kusne is a member of the class of 2018. She completed her PhD in Neuroscience prior to starting medical school at ASU/BNI where she studied the complex signaling mechanisms of glioblastoma. Her passion lies in finding ways to incorporate research and medicine. She has four rescue dogs (yes, four) -- who she loves more than life and thinks of as her children.