“Sttttep right up! Step right up! Ladiiiiesss and gentlemen! Children of all ages! Prepare to be amazed! For you are about to witness a test of dexterity, a challenge to gravity, a feat SO GRAND, you’ll be holding your breath and clutching your seats before you can spell the word ‘cotton candy’.
You may have heard whispers of the Deadline Devil, glimpsed the Anxiety Acrobat, or heard the cackling echoes of the Stress Jester!
[drummmmrolllllllll]
I’m thrilled to introduce, LIVE and in person, please, put your hands together and welcome the beautiful, the daring, the extraordinary….
[trumpet fanfare!]
The Teetering Stressed-Out Fourth-Year Medical Student and Her Trigger Point Troupe!!!!!!”
Now here is where I imagine a thunderous roar of applause as I take to the ring and begin my juggling act of endless to-do list tasks in one hand, interview preparations in the other, whilst balancing on a table of shifting schedules that rotates on two continuously spiraling questions:
“Where will I match???”
“…will I match?”
I know, impressive, isn’t it? Don’t worry, if you missed the first show, I’ll be here for the next several months. And I’m not the only one performing these insane juggling-balancing acts. We all are, because Life. Is. Hard. No matter what stage of it you’re in. Some seasons are harder than others, and if you’re like me, you’ve probably started to notice some physical manifestations of all the stress. Headaches, jaw pain, a stiff neck and tight shoulders. When you go poking around trying to relieve a little bit of it, you may find a spot or two that cries “ow!”, and not in the hurts-so-good massage-type of way.
These overly sensitive, hyperirritable spots of skeletal muscle are myofascial trigger points, or TrPs for short.1 Numerous theories on the formation of TrPs exist, but the most widely accepted is Travell and Simons’ Integrated Trigger Point Hypothesis.2 Please bear with me as I speed through a mini-biochem lesson. The hypothesis is that an inciting injury and/or overloading of the muscle kicks-off a cascade of events. Hypoperfusion from local capillary constriction leads to ischemia and further muscle injury. Biochemicals that sensitize nociceptors (aka pain receptors), like substance P, calcitonin gene-related peptide, prostaglandins, and bradykinin are released, which generate pain signals. Norepinephrine is also released, binding to adrenergic receptors that activate the sympathetic fight-or-flight response. The local hypoperfusion also produces hydrogen ions that create an acidic pH environment that inhibits acetylcholinesterases. Without this, acetylcholine remains available, and miniature end-plate action potentials perpetuate. This means that sarcomeres, the functional unit of muscle, remain in a constant state of contraction.2
The deficient oxygen delivery to the tissue also means aerobic respiration cannot occur, which severely diminishes the amount of ATP available. Without sufficient levels of ATP, calcium cannot be pumped back into the muscle for storage, and sarcomeres remain bound in sustained contraction.2 Altogether, you get taut bands of muscle embedded with knots of contracted trigger points. These may be spontaneously painful, as well as highly sensitive to palpation (hyperalgesia) and stimuli that are normally considered to be non-painful (allodynia).1,2 Not only that, but because the muscle cannot relax, it cannot function optimally, causing poor biomechanics (ie weakness, limited range of motion).
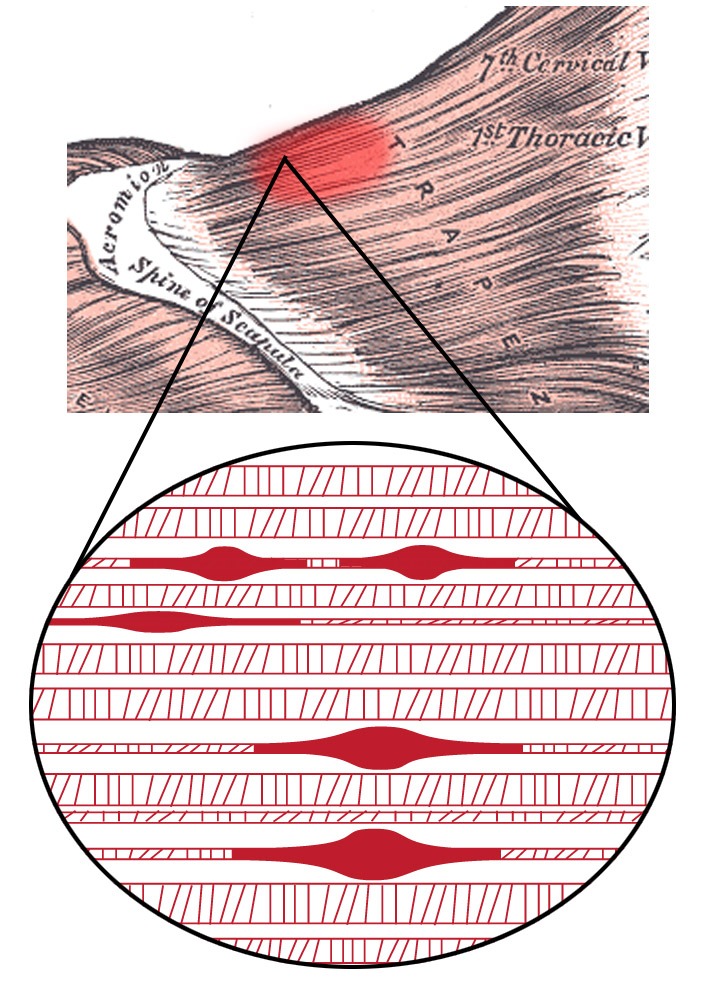
Fig. 1- Illustration of the trigger point complex
TrPs are part of the eight clinical characteristics used for diagnosis of myofascial pain syndrome, listed out in Fig. 2. One of the key features of TrPs is its distribution of pain. The patient will typically be able to identify the most intense area of pain with one finger and endorse a referral pattern upon palpation over the trigger point, as illustrated in Fig. 3.3
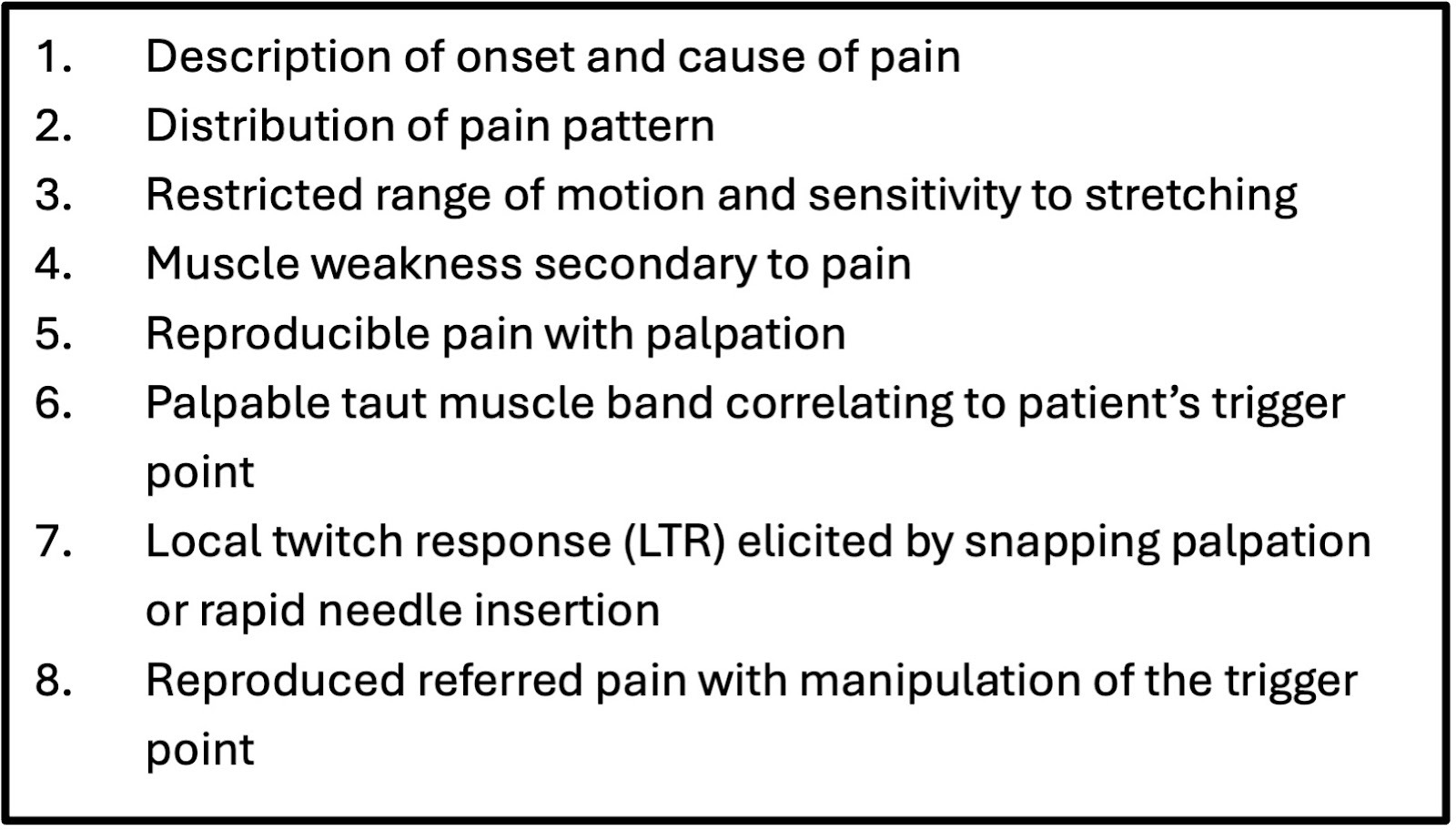
Fig. 2- Clinical characteristics of myofascial pain syndrome/trigger point
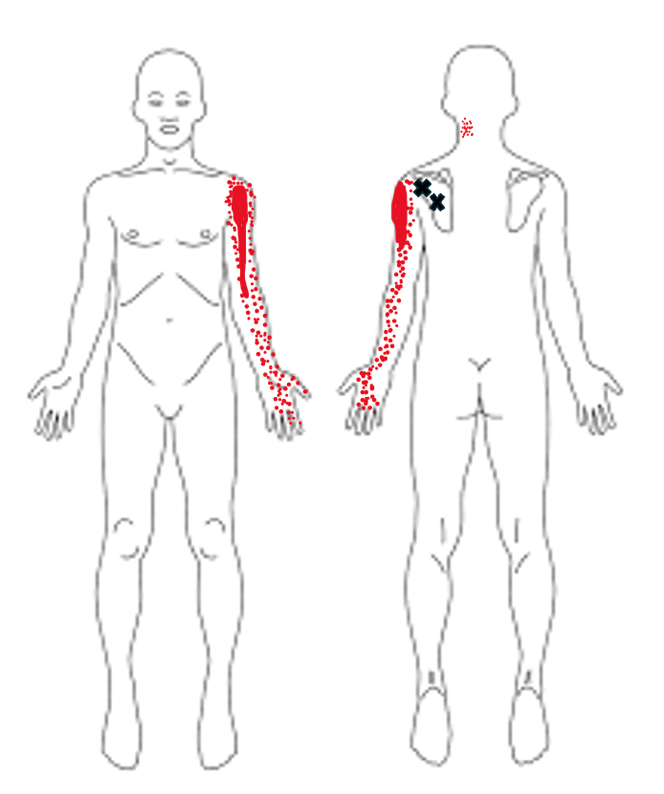
Fig. 3- Example of infraspinatus trigger point referral pattern. X denotes the trigger point, and areas of red the distribution of referred pain. The darker the red, the more intense the pain.4
So, where does stress come into play? The theory of TrPs begins with an inciting injury and/or overloading of muscle. Muscle tension is a reflex to stress, a way for our body to physically guard against anticipated pain and injury.5 When paired with things like poor posture and ergonomics (oh-so-common in our age of screens), muscles are placed under significant strain as they work to counteract and maintain proper alignment. Eventually, they become overloaded, and voilà, trigger points and poor biomechanics ensue.
So, ways to address TrPs. Non-invasive options with massage and physical therapy (PT) for manual work and strengthening are first line. Transcutaneous electrical stimulation (TENS) can be an adjuvant to this. Travell and Simons also advocated for the “spray and stretch” technique. The muscle is passively stretched to its full range of motion after a vapocoolant spray is applied to the trigger point and entire length of the pain reference zone. Another technique is ischemic compression therapy, wherein external compression is applied to the trigger point, creating local ischemia that ablates it.3
Invasive treatments may be second-line or used in conjunction with non-invasive strategies. Trigger point injection with a local anesthetic, corticosteroids, or a combination of the two is common to bring relief and allow for optimal participation in PT programs. Acupuncture or dry needling can also be effective. Complications from these invasive techniques can arise though, such as bleeding, bruising, and infection.3
“Ladies and gentlemen, wasn’t she just INCREDIBLE?! Let’s hear one more round of applause! We thank you for attending our show and being such a great crowd. As always, remember the information shared above is for educational purposes only. Please consult your healthcare provider about individualized treatment options for any myofascial pain and stress.
And don’t miss tomorrow’s performance when Ms. LeFiles and the Troupe add cooking holiday dishes with open flames to the act! Thank you, and have a spectacular evening!”
Disclosures
ChatGPT AI was utilized for the generation of the leading article image.
References
1. Myofascial pain | pm&r knowledgenow. March 6, 2017. Accessed November 15, 2025. https://now.aapmr.org/myofascial-pain/
2. Simons DG, Travel JG, Simons LS. Travel and Simons, Myofascial Pain and Dysfunction: The Trigger Point Manual Volume 1: Upper Half of Body. 2nd ed. Baltimore, MD: Williams & Wilkins; 1999.
3. Lavelle, ED, William Lavelle, and Howard S Smith. “Myofascial Trigger Points.” The Medical clinics of North America 91.2 (2007): 229–239.
4. The trigger point & referred pain guide. Accessed November 16, 2025. http://www.triggerpoints.net/
5. Stress effects on the body. Accessed November 16, 2025. https://www.apa.org/topics/stress/body

Kathleen LeFiles is a medical student from the Class of 2026 at The University of Arizona College of Medicine - Phoenix. She graduated in 2020 from The University of Arizona in Tucson with a degree in Physiology and a minor in Care, Health, and Society. When she's not studying or writing, Kathleen enjoys practicing Pilates and yoga, frequenting local coffee shops, and listening to pop music. Feel free to contact her @kathleenlefiles on Instagram or email at klefiles@arizona.edu.