Sometimes a patient ‘introduces’ themselves before you even see them. From where we were in the hallway of Banner University’s cardiac floor, a resounding tempo stood out amidst the usual noise of a hospital, and the Hospitalist was approaching it.
He told me the patient we’d be visiting had a total artificial heart (TAH), which inspired a plethora of questions. I had the faintest idea of what a TAH was, nevermind how that thumping sound seemed to spill out of the room. That sound manifested from a system of pulsatile hydraulics that allows for propulsion of blood through artificial ventricles. The patient’s own atria and relocated great vessels are connected to these ‘new’ synthetic ventricles, with the TAH now serving as a bridge for eventual heart transplantation.
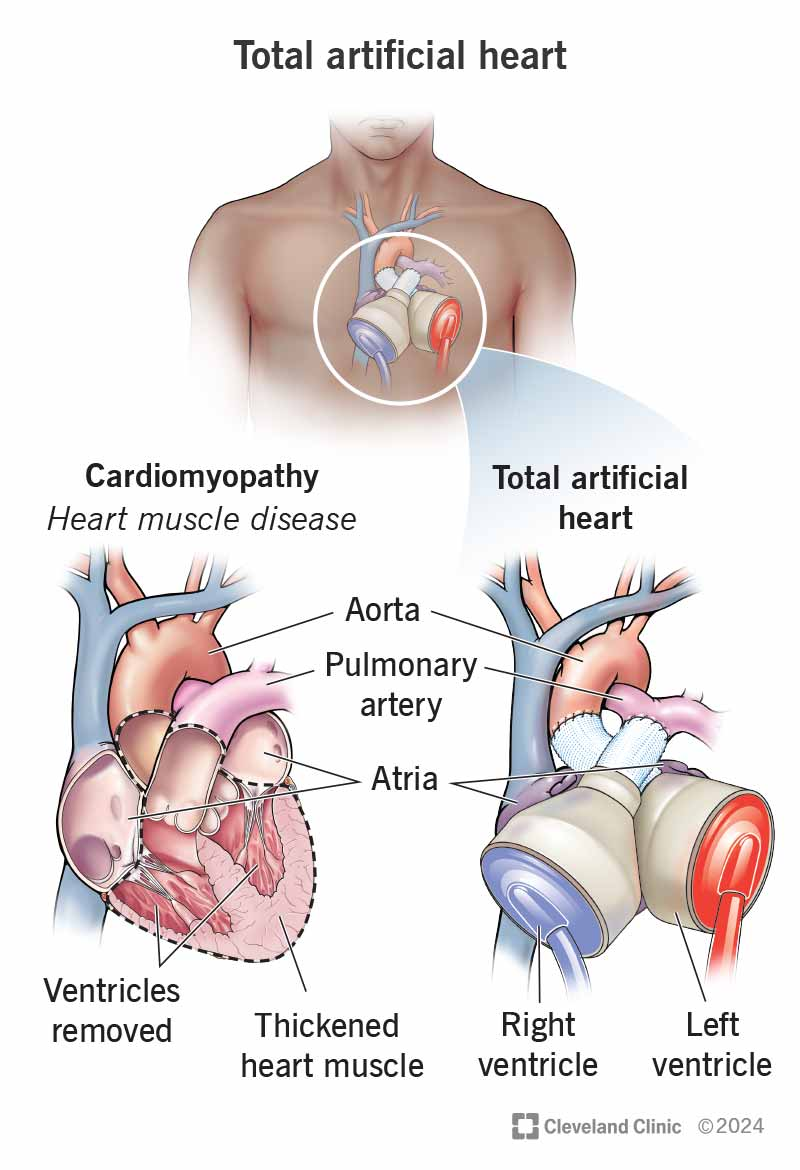
Figure 1. To place a TAH, the procedure first consists of removing the ventricles, valves, and portions of the aorta and pulmonary artery. The TAH is then connected to the patient’s own atria and what remains of their major arteries.
A nurse was stationed by the door, analyzing a monitor, one of several. After dawning the appropriate PPE, I followed in after the Hospitalist, eager to deepen my knowledge.
Flanked by ivory-white machines, towering and obscuring the patient, we stand at the foot of the bed. The patient placed his book aside as the Hospitalist inquired about his progress. He examined as he listened to his story for himself. He auscultated, and with a pause, he asked, amidst the beeping and ringing orchestra, if I could listen. I echoed the question myself and calculated the best place to stand, anxious of the tubes, wires, and potential consequences of faulty proprioception.
He adjusted his gown, looked towards the window, and kindly waited.1
I landed the stethoscope onto his chest. At 130 beats per minute, clear as a voice, dun-dun-dun-dun-dun, a mechanical percussion. Each whirring sound impatiently rushed by another, reliably keeping time. No familiar rhythm to be found, no landmarks, just the looping sound of a pneumatic system driving blood through enclosed polyurethane mesh and out to the body.
As we said our goodbyes, it was as if I had witnessed science fiction, replaying the sound of their ‘heart’-beat in my head. I was offered the chance to ask questions, I asked a few clinical ones.
“How do they sleep with that noise?” I said in passing as the thumping sound dampened the further we walked down the hall.
The Hospitalist laughed, “you have to!”
He’s right, of course, patients adjust and learn, as is the very nature of humans. The ability to adapt is as remarkable as the force of innovation. This is the new normal: taking mediations, scheduling appointments, making lifestyle changes, and most importantly, living with the hope that this is temporary.
Where better to realize this new normal than a place where such it occurs? Bustling with patients and staff and loved ones visiting—people rushing in and out of the hospital, making change happen, or experiencing it themselves.
There is also something to be said about the force of invention, of course.
***
Modern progress regarding artificial hearts can be traced back to the 1920’s, where theory was placed into action through the efforts of renowned physician Alexis Carrel, who earned a Nobel Prize for his work on vascular innovations and advancements towards organ transplantation. His contributions regarding artificial hearts were not solely on his own, but relied on the ingenuity of Charles Lindbergh2. Lindbergh created blood pumps in response to Dr. Carrel’s concerns of how a heart pump could support a patient while in surgery, and successfully created functional pumps a few years later. Their goal expanded to profusing organs when they were removed from the body as an external pump.
The development of the TAH was made possible through decades of innovation from physicians and scientists that persisted for the common goal of saving lives, truly believing that these deaths could be prevented with the right invention. They were right.
The first human TAH was placed by Dr. Denton Cooley in 1969, in collaboration with Dr. Domingo Liotta, who provided his advancements on the artificial heart. This success was short-lived. Due to complications that were never before seen, the patient eventually required a donor heart which later led to their death secondary to the effects of anti-rejection treatment. Permanent artificial hearts were placed in 1982 in several recipients with varying success. With time, this product would change names, design, and ownership, and in the 90’s, MedForte Research formed a partnership with none other than our own University Medical Center in Tucson3.
In 2010, the TAH as we know it today was released. Known as the SynCardia Temporary4, it provided freedom to patients, allowing them to live (relatively) normally and to not be confined to the hospital through the use of a portable freedom driver. This allows for the driver component of the TAH to be carried around, such as in a backpack, allowing patients to resume to their usual level of mobility.
***
Machines only take us so far, but the goal of recovery and persistence is done by the patients, with the support of family and many members of the healthcare staff. It is undeniably worth mentioning the importance of rehabilitation, facilitating their what-ifs and their future quality of life, with the specialty of PM&R guiding patients to their goals.
The practice of medicine is a force of change, on innovation, on our patients, and on ourselves. And then there is the matter of adapting, and hopefully thriving.
Footnotes
- More than 3,400 Americans wait for a new heart each year. ↩︎
- Yes, that Charles Lindbergh, who also went on to create the centrifuge and receive a Pulitzer prize, in addition to his transatlantic legacy. ↩︎
- It was known then as the CardioWest TAH. ↩︎
- As in, serving as temporary until there was a donor heart. ↩︎
Sources
- Clinic C. Artificial Heart. Cleveland Clinic. Published September 7, 2023. https://my.clevelandclinic.org/health/procedures/22173-total-artificial-heart
- Copeland JG. SynCardia Total Artificial Heart: Update and Future. Texas Heart Institute Journal. 2014;40(5):587. https://pmc.ncbi.nlm.nih.gov/articles/PMC3853833/
- Gerosa G, Scuri S, Iop L, Torregrossa G. Present and future perspectives on total artificial hearts. Annals of cardiothoracic surgery. 2014;3(6):595-602. doi:https://doi.org/10.3978/j.issn.2225-319X.2014.09.05
- Health Resources & Services Administration. Organ donation statistics. www.organdonor.gov. Published May 2025. https://www.organdonor.gov/learn/organ-donation-statistics
- Khan S, Jehangir W. Evolution of Artificial Hearts: An Overview and History. Cardiology Research. 2014;5(5):121-125. doi:https://doi.org/10.14740/cr354w
- An example of a portable TAH at work: https://www.youtube.com/watch?v=i9WUHSJrhm4

Fatemah Alzuhairi
Fatemah Alzuhairi is a UACOMP med student from the class of 2028. She graduated from ASU in 2022 with a degree in biomedical sciences and a minor in history. In her spare time, she enjoys planning creative projects, reading, and drinking copious amounts of Earl Grey tea.