In the span of one day, an average adult will take anywhere from 22,000 – 24,000 breaths. And yet how many of those breaths do we actually take notice of? Personally, I only really pay attention when I’m in pilates trying to “hhhaaa” my breath while keeping my legs elevated, spine in neutral, rib cage closed, neck and shoulders off the floor, pumping my arms to the beat of the music as the instructor stands at the front of the room wearing a headset circa Britney Spears, counting in a voice better suited for a flight attendant than a fitness instructor in class where my muscles feel as though they are simultaneously turning into Jell-O and being scorched by the Phoenix summer sun…..
If you failed to notice that you took about 3-4 breaths while reading that run-on sentence, or maybe unknowingly held your breath like I did, well then you’ve just answered my previous question. We hardly, if ever, pay attention to our breathing, but that’s how our bodies were designed after all. Respiratory centers in the brain stem, in response to levels of oxygen and carbon dioxide measured by chemoreceptors, send signals via the phrenic nerve to stimulate the diaphragm without a single conscious thought on our part.
“Breathing, the process of taking air into and expelling it from the lungs, is caused by a three-dimensional shape change in the thoracic and abdominal cavities” 1
While the brain is the mastermind (pun intended) behind when to inhale and exhale, the diaphragm is the brawn that enforces the necessary shape changes so that air can enter and exit the lungs. Often likened to the shape of a jellyfish or a parachute, the diaphragm is asymmetrically dome-shaped and spans across the torso in the transverse plane to separate the thoracic and abdominal cavities. It is unique in its design in that it connects to and supports itself via a central C-shaped tendon. This distinct shape and structure allows for three-dimensional movement of the diaphragm to alter space through the body during breathing. As a result though, it has much more nuanced origin and insertion sites than a typical muscle, creating mixed opinions and overall confusion on what its primary action is.
To review, origin and insertion sites are where muscle attaches, and are determined by two principals: structure and function. From a structural perspective, proximal points are closer to the body’s core and typically serve as origins, while distal (peripheral) sites are insertions. Functionally, there is more stability the more proximal you are, hence again, a proximal point would be the muscle’s origin because it can anchor it during contraction. These principles work well when thinking about a muscle such as the biceps brachii that runs along a longitudinal axis. It originates at the scapula in the shoulder and inserts close to the head of the radius. When you flex your bicep the muscle contracts upwards towards the shoulder to pull the distal forearm and hand closer to the body’s center.
Figure 1: Bicep Contraction and Relaxation3
Things get much more complicated when thinking about diaphragmatic contraction. During inhalation the diaphragm contracts and flattens downward to compress the abdominal organs and create space for the lungs to expand. Now, traditional anatomy textbooks label the sternum’s xiphoid process, costal cartilages, floating ribs 11 and 12, and lumbar vertebrae as the origin sites2, and the central tendon as the insertion site. At first glance this makes sense, since it appears as though the center of the diaphragm is being pulled down closer to the origin sites. However, I established earlier that origin sites are found proximally. The central tendon lies at the very core of the diaphragm and at the core of the torso…you can’t get more proximal than that. In fact, the heart is anchored to the central tendon via the pericardium and together they have very little mobility. On top of that, the supposed origin sites I listed above are more distal and composed of cartilage, which overall provides less stability than bone.
Upon closer inspection, when the diaphragm contracts, the muscle fibers shorten along the vertical axis to 1) push down the abdominal viscera as previously mentioned, but also to 2) lift the bottom of the ribcage to increase the thoracic cavity space. Both cavities change size simultaneously around the central tendon that remains fixed in one place. It is because of this complex movement that I pose a challenge to traditional descriptions of diaphragmatic anatomy. Risky perhaps, but I also think it’s helpful when trying to understand the anatomy and the dynamics of breathing. Instead of thinking of typical origin and insertion sites, it is much simpler to think of the diaphragm as having upper and lower attachments. The diaphragm’s central tendon acts as the upper attachments while the xiphoid process, costal cartilages/ribs, and lumbar vertebre serve as the lower attachments. Overall, this fabricates a unique and powerful muscle that supports itself.
Figure 2: Diaphragm Contraction and Relaxation4
Phew, okay, that was a lot I just covered. I’m hoping at this point you’re still with me, and didn’t get too lost in the twisting maze of origins, insertions, proximal points, and distal points I created. Let’s just….pause and take a deep breath. It may be the only one you think about today.
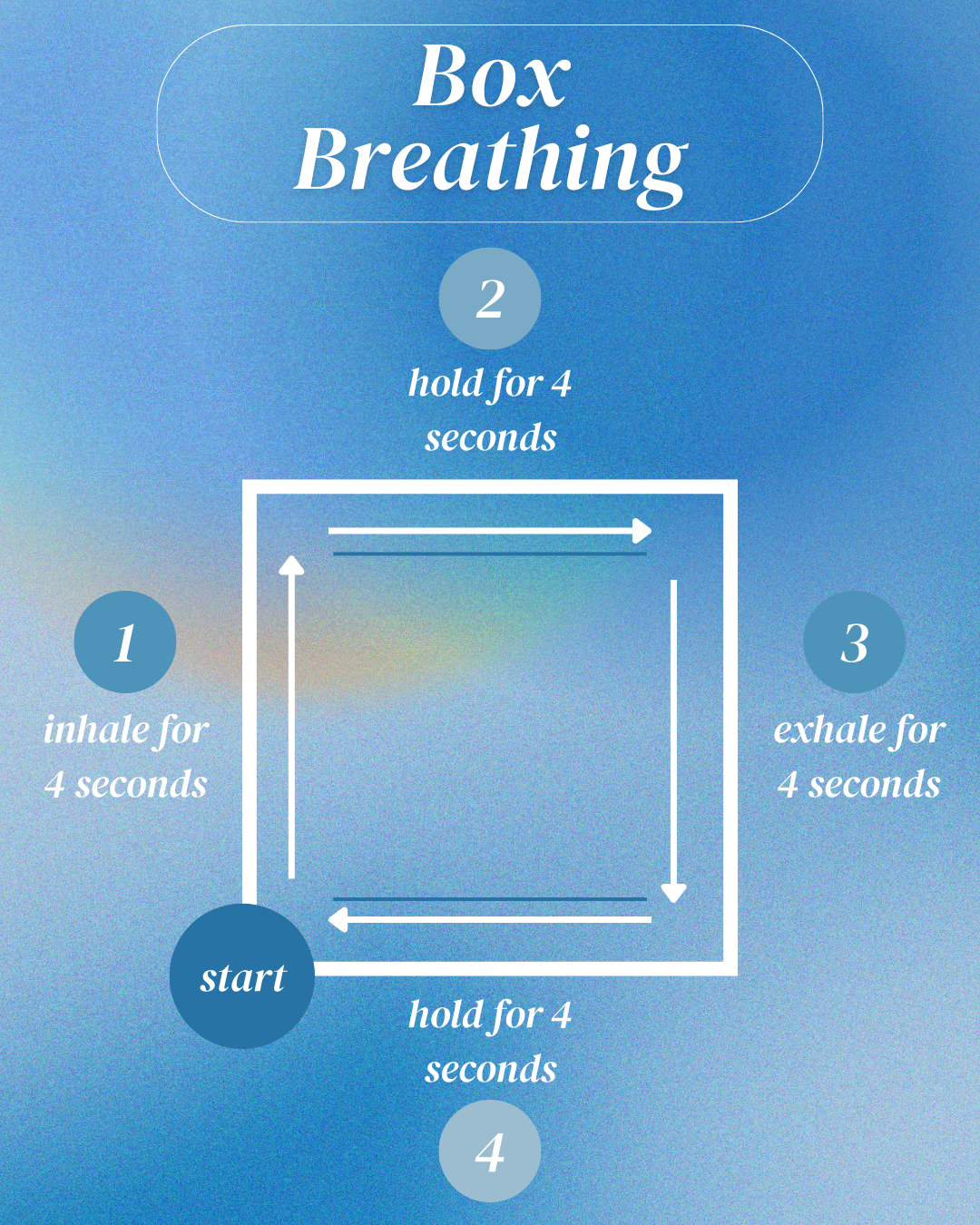
Figure 3: Basic box breathing exercise
References
- Kaminoff, Leslie; Matthews, Amy. Yoga Anatomy. Human Kinetics, 2007.
- Radiopaedia.org
- Wikimedia Commons
- MakeaGIF

Kathleen LeFiles is a medical student from the Class of 2026 at The University of Arizona College of Medicine - Phoenix. She graduated in 2020 from The University of Arizona in Tucson with a degree in Physiology and a minor in Care, Health, and Society. When she's not studying or writing, Kathleen enjoys practicing Pilates and yoga, frequenting local coffee shops, and listening to pop music. Feel free to contact her @kathleenlefiles on Instagram or email at klefiles@arizona.edu.