The treatment of intervertebral disc herniations vary widely, from conservative to invasive modalities. A common surgical procedure that is performed to manage this pathology is a microdiscectomy, where the extruded disc material is removed. In the lumbar spine alone, over 300 thousand lumbar microdiscectomies are performed in the United States each year.1,2 While this procedure has a success rate of up to 90%, it is not without the risk of complications.3
One of the most common complications of discectomy surgery is disc reherniation. The lumbar disc herniation recurrence rate post-discectomy ranges from 5-15% and is a large driver of reoperation.4
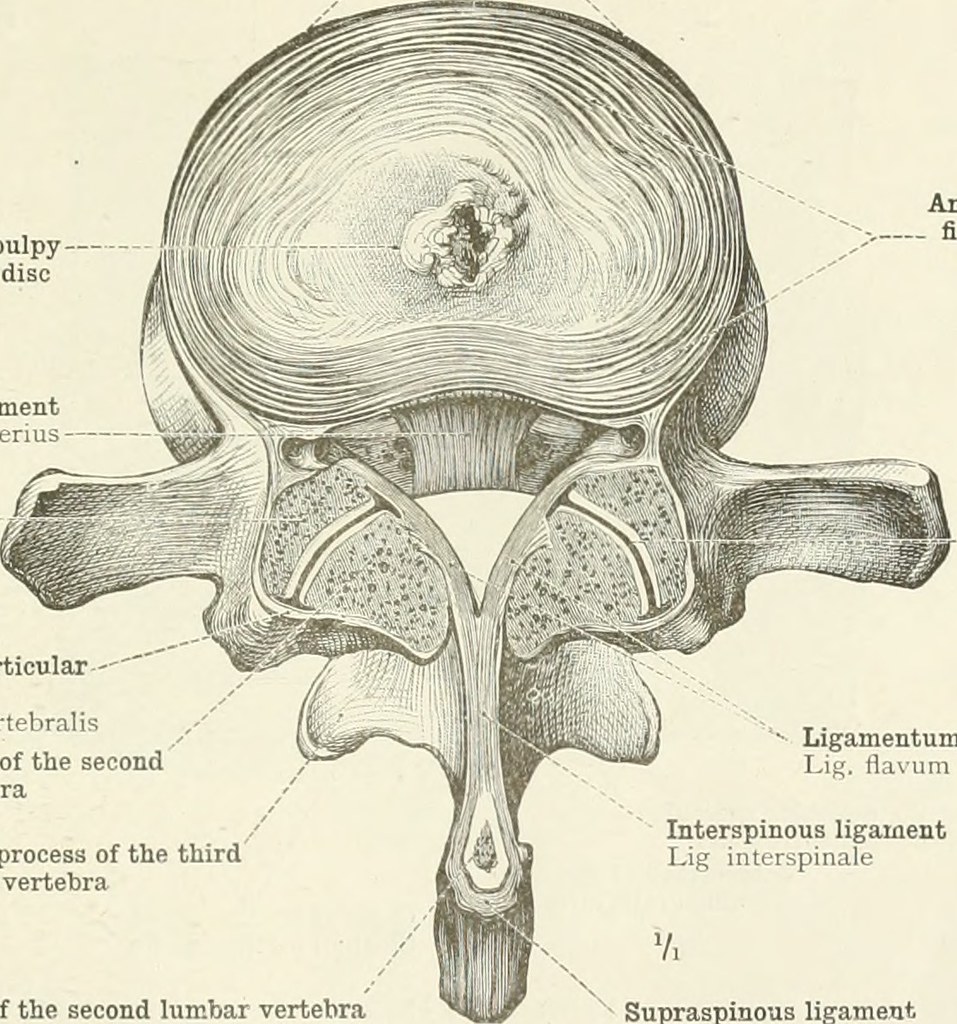
Disruption of the annulus fibrosus, the dense collagen structure that surrounds the proteoglycan-rich nucleus pulposus can occur following trauma or age-related spinal degeneration.5 Traditional microdiscectomy doesn’t involve repair of the annulus, which has led researchers to explore options for repair of the annulus fibrosus following microdiscectomy using combinations of adhesives, mesh devices, and tissue repair systems.6
A research group in the Departments of Orthopedics and Bioengineering at University of Pennsylvania published a research article in Science Translational Medicine in November attempting to address the shortcomings of the current state of technology surrounding annulus fibrosus repair. This was a combined in vitro and in vivo study to determine the efficacy of a nanofiber patch device with tension-activated microcapsules in its ability to repair the functionality of the annulus, while simultaneously reducing the downsides of inflammation due to the procedure.7
The tension-activated repair patches (TARPs) used in this study are designed to integrate into normal tissue using a scaffold-like nanofiber structure that can mimic the dynamic stability of the annulus fibrosus. Built into this scaffold are pockets of microscopic capsules that are designed to be released in response to tension and deformation.7 Inside the mechanically-activated microcapsules (MAMCs) is anakinra, a biologic drug that blocks the receptor for IL-1β, a key mediator of the inflammatory response.8
The homologous structure of the nanofiber patches, combined with the microcapsules of anakinra, showed great promise in the in-vitro results of the study. Through serial tensioning tests, the researchers found that drug delivery rate can be altered with small changes in the microarchitecture of the repair patches. They also discovered that MAMC-delivered anakinra inhibited the upregulation of matrix metalloproteinase-3 and lipocalin-2, demonstrating that anakinra attenuates catabolic signaling caused by IL-1β.7 Decreasing the downstream effects of IL-1β could potentially reduce back pain associated with disc injury, as well as preventing re-herniation.
Once the in-vitro study was complete, the researchers transitioned into an in-vivo study using a goat cervical spine model for annulus fibrosus tear, since goats have cervical spine morphology similar to humans. The researchers induced a full-thickness annular tear in the C2-3 and C3-4 levels of 8 goats, and then repaired one level with either the TARP+anakinra, or the TARP+control. The adjacent level was used as a nonoperative control.7
The researchers then used imaging and histological studies to assess the tissue at 4 weeks postoperatively. Overall, the TARP procedure helped retain the nucleus pulposus, reinforced the annulus fibrosus, and prevented disc-wide remodeling and tissue necrosis that’s seen following annular tear and disc herniation. The TARP+anakinra prevented inflammatory remodeling at the site of TARP implantation, which is a common reaction to foreign body implantation. The drug’s delivery also showed via histological analysis, as well as imaging, that disc architecture was similar to uninjured controls.7
The promise lies in the potential to restore the tensegrity of the dense annulus to pre-injury levels, while also preventing the inflammatory response associated with tissue injury and foreign body implantation. These findings suggest a potential solution to address the limitations inherent in traditional discectomy surgery.
Although these data are promising regarding the development of technology involved in annulus repair, there are many limitations of this technology that would likely manifest when translated to clinical use.
First, the TARP must be sutured in place, which presents many technical challenges, in addition to the added risks of increased operative time. Second, this study used a model for anterior disc herniations of the cervical spine due to the easy access in the animal model that they used. The vast majority of disc herniations occur in the posterolateral aspect of the intervertebral disc, where the annulus lacks structural support.9 The added technical challenge associated with accessing this area of the spine may lead to challenges that outweigh the benefits of the technology.
The last consideration to be made involves the researchers’ model of disc herniation. The protocol required direct repair with the TARP immediately following the induced annular tear. It is important to highlight that most individuals attempt conservative measures (i.e. physical therapy or injections) before progressing to surgery, however, this model could be most useful in the population of patients with acute spinal cord injury following disc herniation. The data in these patients suggest early operation is preferred,10 and could be applicable to the conditions of the study highlighted in this paper.
Regardless, the findings out of UPenn’s orthopedics department are promising for the technology surrounding annular tear repair following discectomy. Further studies are imperative before making assumptions about the application of this technology in humans.
References
1. Aljoghaiman M, Martyniuk A, Farrokhyar F, Cenic A, Kachur E. Survey of lumbar discectomy practices: 10 years in the making. J Spine Surg. 2020;6(3):572-580. doi:10.21037/jss-20-519
2. Daly CD, Lim KZ, Lewis J, et al. Lumbar microdiscectomy and post-operative activity restrictions: a protocol for a single blinded randomised controlled trial. BMC Musculoskeletal Disorders. 2017;18(1):312. doi:10.1186/s12891-017-1681-3
3. Atlas SJ, Deyo RA, Keller RB, et al. The Maine Lumbar Spine Study, Part II. 1-year outcomes of surgical and nonsurgical management of sciatica. Spine (Phila Pa 1976). 1996;21(15):1777-1786. doi:10.1097/00007632-199608010-00011
4. Shimia M, Babaei-Ghazani A, Sadat BE, Habibi B, Habibzadeh A. Risk factors of recurrent lumbar disk herniation. Asian J Neurosurg. 2013;8(2):93-96. doi:10.4103/1793-5482.116384
5. Tenny S, Gillis CC. Annular Disc Tear. In: StatPearls. StatPearls Publishing; 2023. Accessed November 24, 2023. http://www.ncbi.nlm.nih.gov/books/NBK459235/
6. Choy WJ, Phan K, Diwan AD, Ong CS, Mobbs RJ. Annular closure device for disc herniation: meta-analysis of clinical outcome and complications. BMC Musculoskeletal Disorders. 2018;19(1):290. doi:10.1186/s12891-018-2213-5
7. Peredo AP, Gullbrand SE, Friday CS, et al. Tension-activated nanofiber patches delivering an anti-inflammatory drug improve repair in a goat intervertebral disc herniation model. Science Translational Medicine. 2023;15(722):eadf1690. doi:10.1126/scitranslmed.adf1690
8. Lopez-Castejon G, Brough D. Understanding the mechanism of IL-1β secretion. Cytokine Growth Factor Rev. 2011;22(4):189-195. doi:10.1016/j.cytogfr.2011.10.001
9. Dydyk AM, Ngnitewe Massa R, Mesfin FB. Disc Herniation. In: StatPearls. StatPearls Publishing; 2023. Accessed November 24, 2023. http://www.ncbi.nlm.nih.gov/books/NBK441822/10. Badhiwala JH, Wilson JR, Witiw CD, et al. The influence of timing of surgical decompression for acute spinal cord injury: a pooled analysis of individual patient data. Lancet Neurol. 2021;20(2):117-126. doi:10.1016/S1474-4422(20)30406-3
Benson Lagusis is a member of the University of Arizona College of Medicine - Phoenix Class of 2026. He graduated with a B.S. in Exercise Science from Northern Arizona University before earning a Master's degree in Biomedical Sciences from Midwestern University. Benson played baseball in college, and is interested in sports medicine and health promotion/education. During his free time, Benson is an avid hiker, reader, and Netflix binge-watcher.